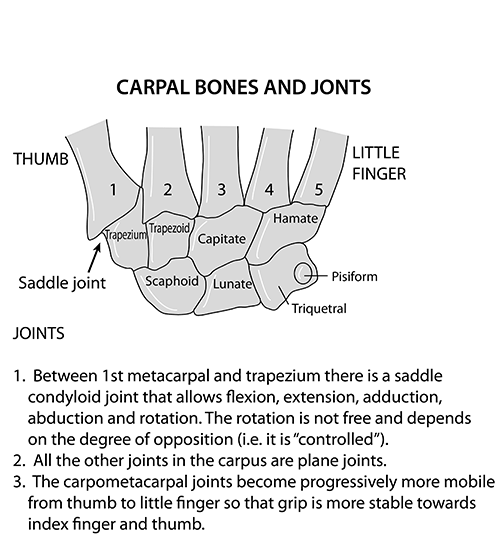
- Ossification Centres of Carpal Bones :
- Capitate: 1-3 months
- Hamate: 2-4 months
- Triquetrum: 2-3 years
- Lunate: 2-4 years
- Scaphoid: 4-6 years
- Trapezium: 4-6 years
- Trapezoid: 4-6 years
- Pisiform: 8-12 years
-
Capitate is the first one and Pisiform is the last one to ossify.
-
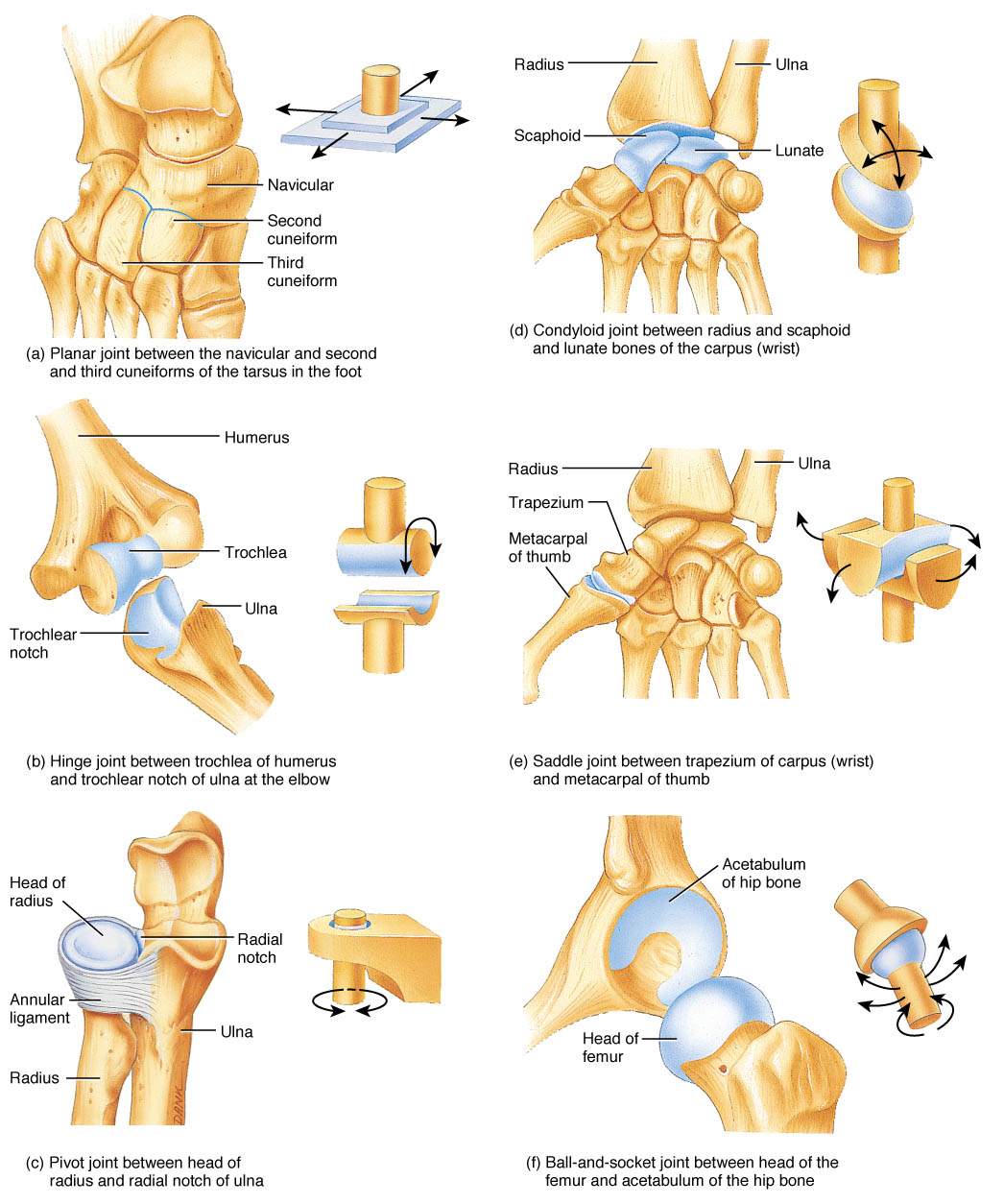
Ball & Socket Joints : (Mnemonic –> THIS)
- T –> TaloCalcaneoNavicular Joint
- H –> Hip Joint
- I –> IncudoStapedial Joint
- S –> Shoulder Joint
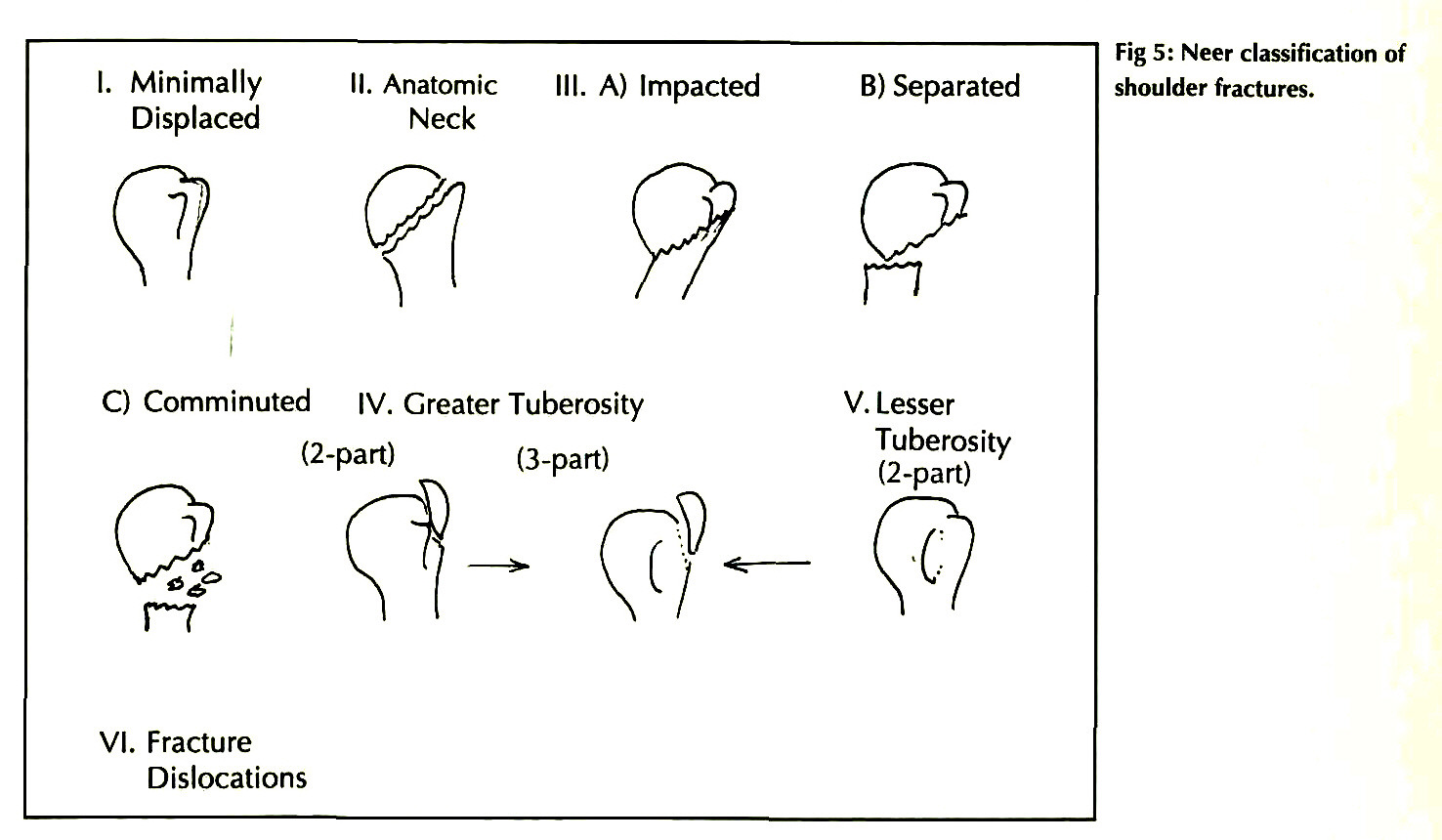
3. The following X-Ray is Type III Fracture Proximal Humerus ( Impacted )

Following is the detail of Neer’s Classification of Proximal Humerus Fracture
4. All of the following are true about Sprengel’s Deformity except :
- Associated with Congenital Scoliosis
- Associated with Diastemetomyelia
- High incidence with Klippel Fiel Syndrome
- Associated with Dextrocardia ( Answer )
Sprengel deformity
It is congenital elevation of the scapula, is a complex deformity of the shoulder and is the most common congenital shoulder abnormality.
Sprengel deformity is usually noticed at birth and has both cosmetic and functional implications. The elevated scapula is visually noticeable and there is an associated restriction in the motion of the scapula and glenohumeral joint.
Associations of Sprengel’s Deformity —
An omovertebral bar (fibrous, cartilaginous and/or osseous connection between the scapula and cervical spine) is often present.
It is also commonly associated with hypoplasia or atrophy of regional muscles, and these associated features can cause further misshaping of the shoulder and limitation of shoulder movement.
Patients with Sprengel deformity often have one or more of the following abnormalities and conditions:
- Klippel-Feil syndrome
- Spina bifida & Diastemetomyelia
- Kyphoscoliosis
- Torticollis
- underdevelopment of clavicle or humerus
5. Question –>
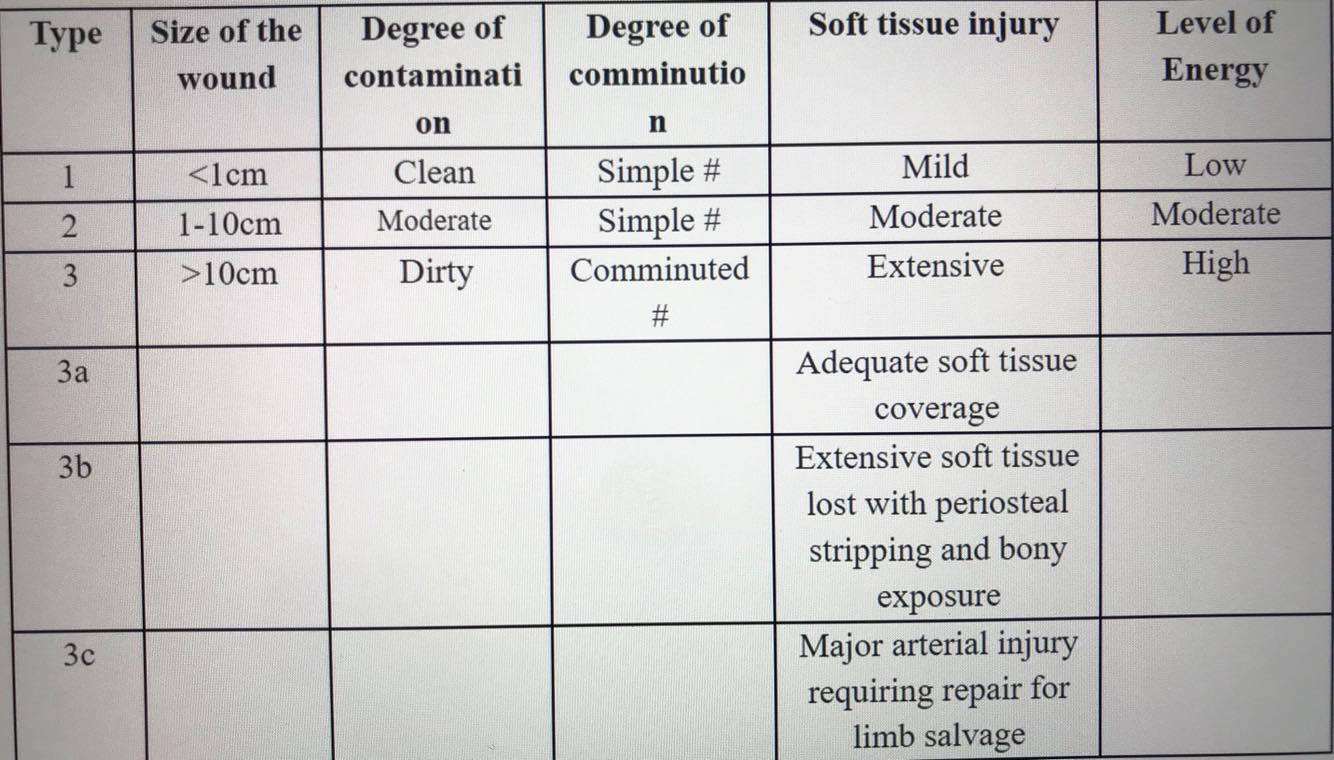
A patient with history of RTA present in ED. Attending orthopedician writes Gustilo’s Type IIIB for his both bones fracture in lower limbs injury. According to Gustilo Anderson Classification what is correct ?
A. B/L limb wound of >10cm with adequate soft tissue coverage inspite of extensive laceration , flaps, avulsion injury & regardless of size of wound
B. B/L limb wound of size <1cm
C. B/L limb wound of size > 10cm with extensive soft tissue damage & periosteal stripping
D. Wound between 1 and 10 cm in length without extensive soft-tissue damage, flaps or avulsions
Answer –> C
6. Question –>
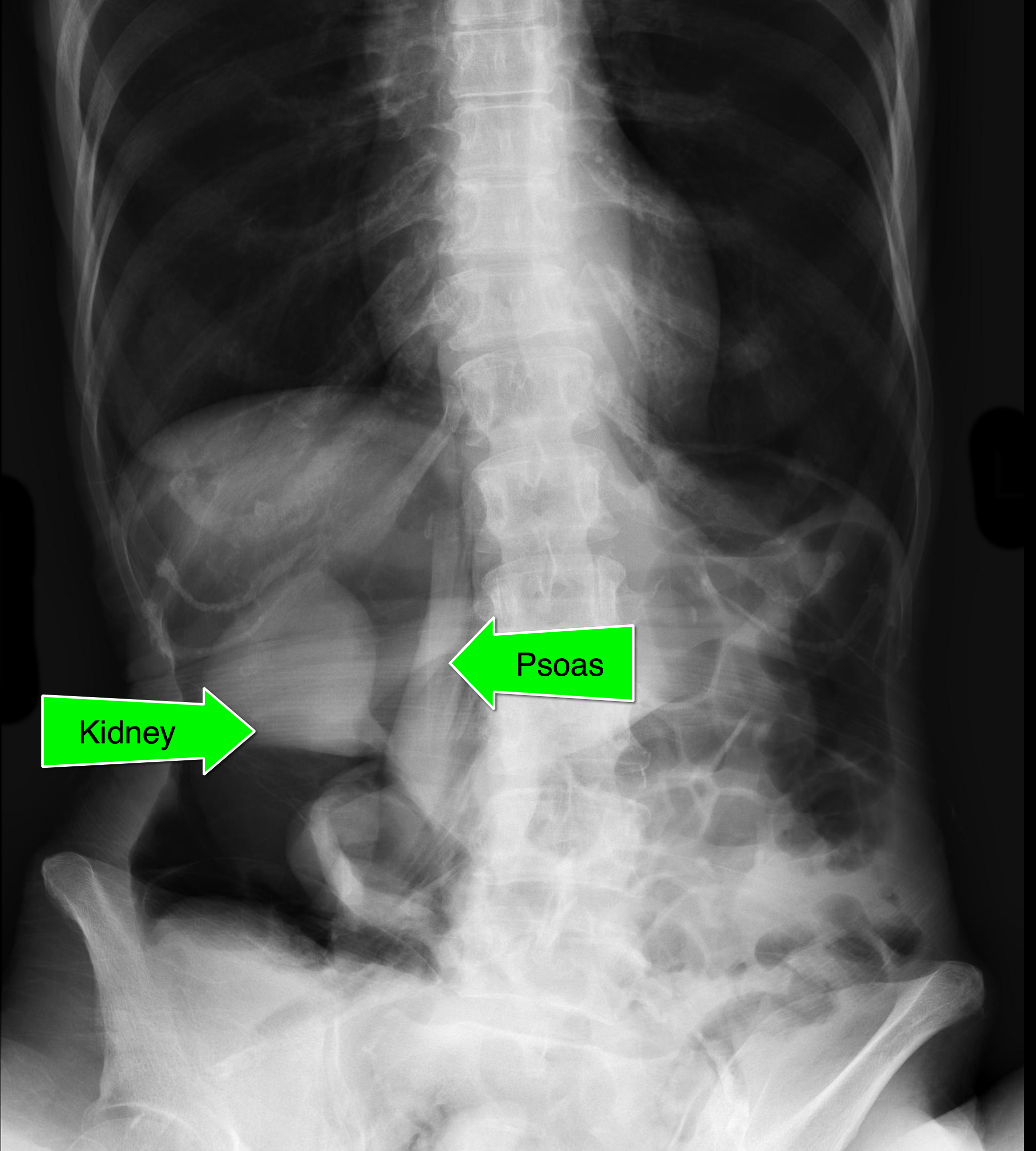
A 10 years old boy with difficulty and pain during walking for the past 10 days. There is no fever currently. On examination right hip is flexed and there is fullness in the the right lumbar region. X ray shows soft tissue shadow in the right side of abdomen. What is the most probable diagnosis?
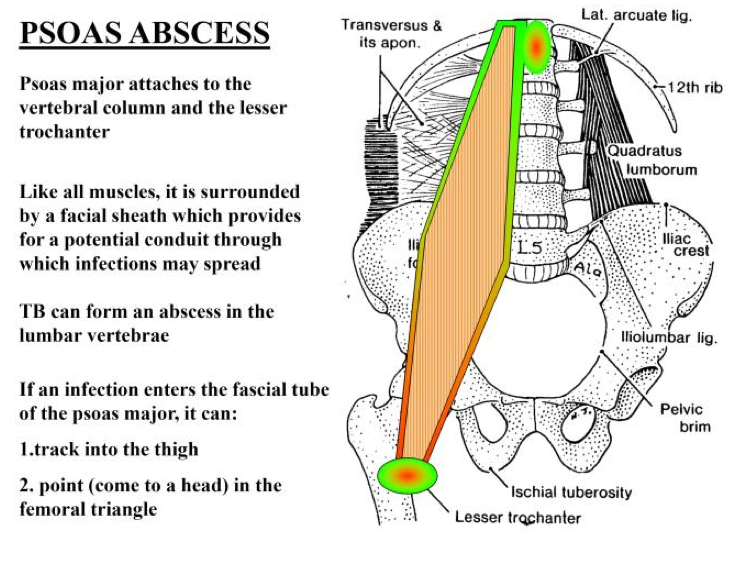
a. Psoas Abscess
b. Testicular Torsion in an Undescended Testis
c. Pyonephrosis
d. Appendicular Lump in RetroCaecal Appendix
Answer –> a
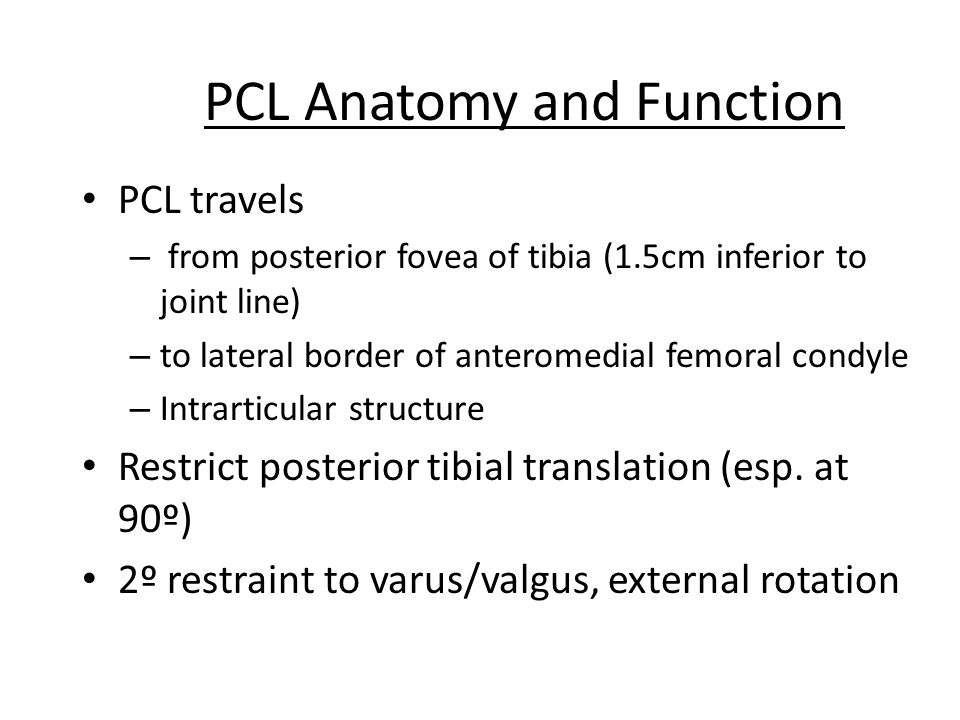
7. Posterior Cruciate Ligament :
– PCL is the only primary restraint to posterior translation throughout the entire knee range of motion (ROM).
– PCL is an Extra Synovial Structure approximately twice as strong and twice as thick as the normal ACL (therefore less commonly injured)
Dimesions :
– Size: 13 mm, its length, 38 mm, (approximates that of ACL);
– Origin:
– PCL originates from the antero-lateral aspect of medial femoral condyle in the area of intercondylar notch;
– Its origin is much more anterior than that of ACL
– insertion:
– Tibial attachment is not intra articular, but over back of tibial plateau, it is approximately 1 cm distal to the joint line
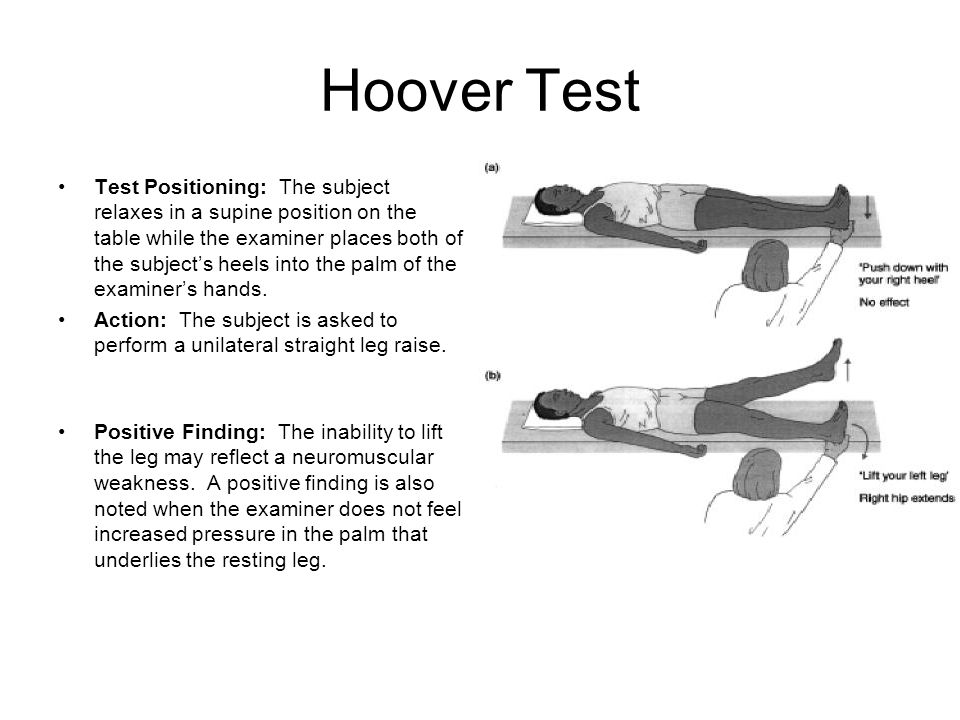
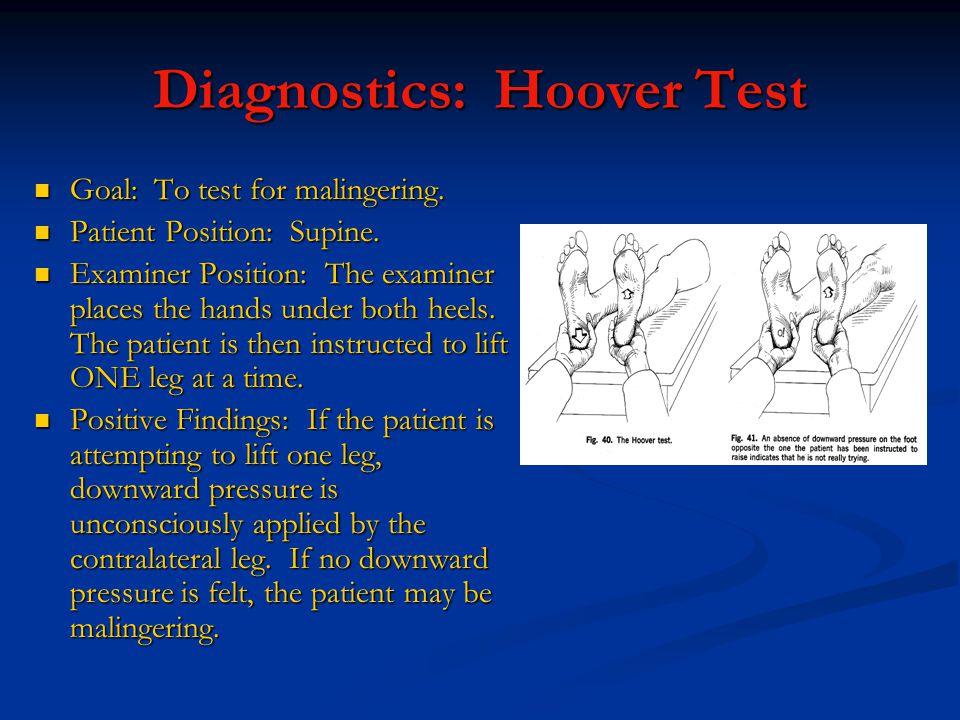
8. A Patient came with complains of lower limb weakness. Examiner places one hand under the patients heel and patient is then asked to raise his other leg against downward resistance. What is the test being performed ?
a. Hoover’s Test
b. Mc Bride Test
c. Waddell’s Test
d. O’Donoghue’s Test
Answer –> a
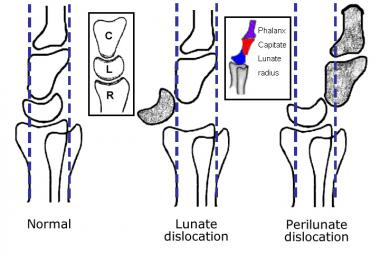
9. Fracture Scpahoid v/s Lunate Dislocation v/s TransScaphoid PeriLunateDislocation
 Fracture Scaphoid
Fracture Scaphoid
 Lunate Dislocation
Lunate Dislocation![]() TransScaphoid PeriLunate Dislocation
TransScaphoid PeriLunate Dislocation
For More Updates on Orthopaedics :
Please Click on the following link –
Leave a Reply to Baby peguCancel reply