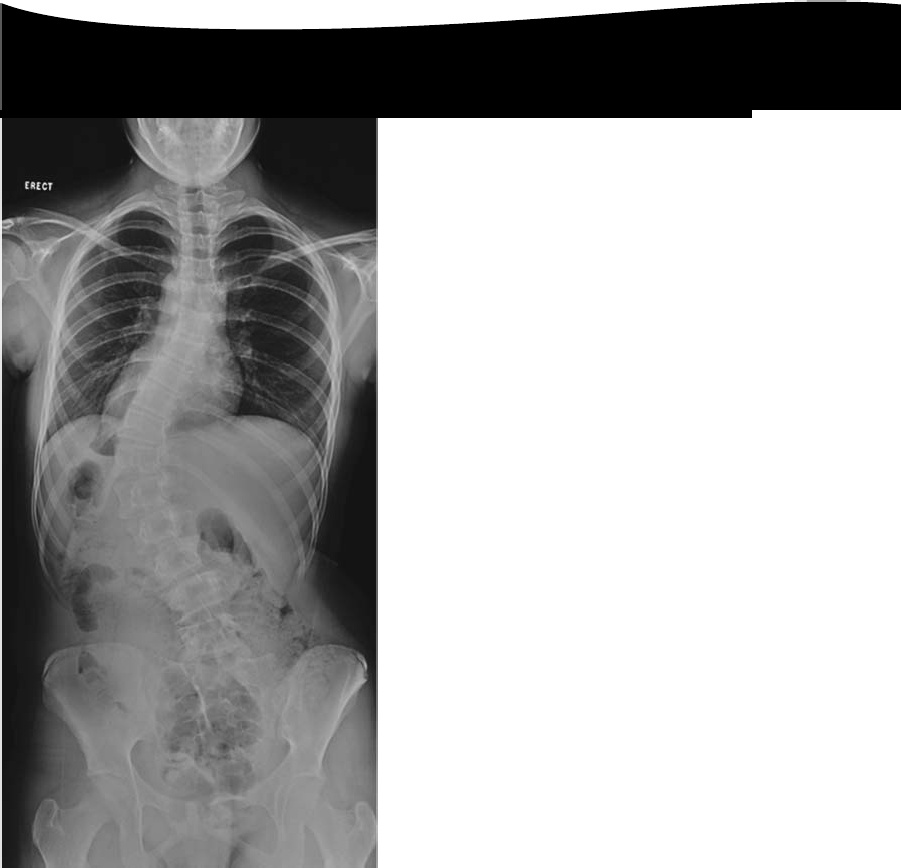

This is idiopathic scoliosis.
It is commonest in girls and often presents around adolescence. The thoracic curve is usually right sided.The prevalence is around 3% of the population, although less than 10% of curves need treatment.
What factors affect progression of the deformity?
-The future growth potential of the patient, i.e. the level of skeletal maturity at the time of diagnosis.This is measured by the Risser stage:
Risser 0 = no ossification of the iliac epiphysis
Risser 1 = 0–25% ossification
Risser 2 = 25–50% ossification
Risser 3 = 50–75% ossification
Risser 4 = 75–?00% ossification
Risser 5 = fused epiphysis
The curve magnitude at the time of diagnosis:
-Curves of <30° at maturity are unlikely to progress
-Curves of 30–50° at maturity are likely to progress another 10–15°
-Curves of >50° at maturity are likely to progress at around 1°/year3.
Sex: curves in females are more likely to progress
Curve type: double curves are more likely to progress
Classifications —
There are two common classification systems.
King and Moe describe Types 1–5 depending on the shape of the curve:
Type1: S-shaped double curve where the lumbar curve is larger or less flexible
Type 2: S-shaped double curve where the thoracic curve is larger or less flexible
Type 3: single thoracic curves
Type 4: long thoracic curves where L4 is tilted into the curve
Type 5: double thoracic curve where T? is tilted into the thoracic curve
The more complex Lemke classification system describes the curve type (1–6) and adds a modifier(A, B, or C) depending on where the lumbar curve is in relation to central sacral vertical line, and another modifier (–, N, or +) based on the thoracic sagittal profile
Leave a Reply